
Are You a Wound Care Detective? Case 1
January 27, 2021
Keywords
Categories
A few weeks ago I introduced you to the concept of how being a wound care professional is often a lot like being a detective (read series introduction post here). This blog post is going to start our “cases.” I decided, in keeping with the theme, to write it up similar to what you would see in a court document. For each case, remember the key objects:
- The what: Looking at the pathophysiology of the wound, what is causing it?
- The why: Focus on why this wound is not healing—are you missing something?
- The when: When did this wound start—did the patient have an accident that caused it?
- The where: Look at where on the body the wound is located—are there any other wounds anywhere?
- The how: Focus on how the wound got to this point and what they have tried in the past.
The One with a Club Sandwich Style Dressing
Facts
Application of multiple dressings with contradictory therapeutic actions resulted in delayed wound healing.
Procedural History
The patient is a 65-year-old man who presented with a stage 3 pressure ulcer/injury to the left ischial tuberosity. He has a history of an anoxic brain injury, is non-verbal, and is unable to move himself. The family reports that the ulcer started after a prolonged car trip. He has a colostomy and a suprapubic catheter. The wound is dry, with minimal exudate, and the periwound skin is fragile and has a slight amount of contact dermatitis. The tissue in the wound bed is mostly adhered slough, with a small amount of granulation tissue. He is being cared for by his family members, who refuse to use any type of bordered foam dressing or hydrocolloid type dressing. Dressings being used included a hydrogel applied directly to the wound base. This dressing is covered with a silver hydrofiber and covered with an absorbent pad, which is secured with cloth tape. The patient has been using this dressing based on information found by “googling.”
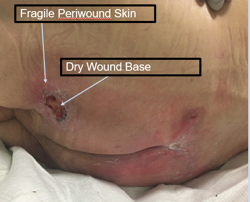 *Photographic Evidence, Copyright Emily Greenstein
*Photographic Evidence, Copyright Emily GreensteinIssue
The main issue with this case goes back to the basics of wound care—appropriate dressing selection to maintain a moist wound healing environment. Starting at the beginning, what is the pathophysiology of this wound? It is a pressure injury/ulcer secondary to immobility and total care. The patient does have a gel cushion in his wheelchair and has been limiting sitting to one-hour intervals three times a day for meals. Next, look at what they have been trying and what has not been working. The family states that they started using the hydrogel because the wound was too dry. They then added the hydrofiber because it was silver and would help with bacteria, and finally, they added the absorbent pad to collect drainage and “pad” the wound.
Ruling
Guilty of misuse of advanced topical dressings.
Application
In this case, the patient and his family were using dressings based on what they had found on the Internet.
Conclusion
Based on the evidence, let’s look at what could have been done differently. When deciding on dressing selection, look at the needs of the wound.
- What phase of healing is the wound in? In this case, the wound was stuck in the chronic inflammation state.
- How much exudate is there, and what does it look like? The wound presented was dry, with little exudate. There was adhered slough with minimal granular tissue present.
- What is the condition of the surrounding skin? The periwound skin was broken down as a result of irritation from the dressings.
- Where is the wound located? It was located on a pressure point.
- Is there contamination or any infection present? At this time, stool and urine were contained away from the wound, and there were no signs of infection.
- What is the depth of the wound, and are there any exposed structures? There were no exposed structures within the wound base. Deep partial-thickness skin loss was noted.
- Is there any tunneling or undermining? No undermining was noted.
- Are there any skin sensitivities? The family stated that he reacted to hydrocolloids in the past.
- What is the patient’s age? As we age, the skin undergoes both structural and biochemical changes, as well as changes in neurosensory status, perception, permeability, response to injury, and repair capacity, and the incidence of some skin diseases is increased.1
- Where is the patient being treated, and what is the level of caregivers? In this case, the patient was being treated at home by his family members, who had no formal medical background or training.
Dressing selection based on exudate level is important. As we discussed previously, creating a moist wound healing environment is of utmost importance. Often I like to think of moisture management like “Goldilocks.” We don’t want it too dry or too wet; we want moisture to be just right.2 When looking at the mechanism of actions related to the dressings that the patient was using, you can see why this combination was perhaps not the best choice.
Hydrogels add moisture to a wound bed and are hydrophobic, meaning they add moisture to the wound bed.3 Hydrofibers (if placed on dry) are designed to wick fluid away from the wound bed and are hydrophilic, meaning they pull moisture into them.3 The wound also showed no signs of increased bioburden or infection, so the use of silver would not be indicated. Based on the current state of the wound, the patient’s condition, and the dressing mechanisms, the patient was transitioned to a hydrogel sheet that was changed daily, and the periwound skin was treated with a cyanoacrylate skin protectant. As the wound progressed through the phases of healing, he was transitioned to a petroleum-impregnated gauze dressing, and eventually the wound went on to heal.
References
- Grove GL. Physiologic changes in older skin. Clin Geriatr Med. 1989;5:115.
- Weigand C, Tittelbach J, Hipler U, Elsner P. Clinical efficacy of dressings for treatment of heavily exudating chronic wounds. Chronic Wound Care Manag Res. 2015;2:101-111.
- Wound Source. Dressing types. 2019. https://www.woundsource.com/product-category/dressings. Accessed January 13, 2020.
About the Author
Emily Greenstein, APRN, CNP, CWON, FACCWS is a Certified Nurse Practitioner at Sanford Health in Fargo, ND. She received her BSN from Jamestown College and her MSN from Maryville University. She is certified as an Adult-Gerontology Nurse Practitioner through the American Academy of Nurse Practitioners. She has been certified in wound and ostomy care through the WOCNCB for the past 8 years. At Sanford she oversees the outpatient wound care program, serves as chair for the SVAT committee and is involved in many different research projects. She is an active member of the AAWC and currently serves as co-chair for the Research Task Force and Membership Committee. She is also a working member of the AAWC International Consolidated Diabetic Ulcer Guidelines Task Force. She has been involved with other wound organizations and currently serves as the Professional Practice Chair for the North Central Region Wound, Ostomy, and Continence Society. Emily has served as an expert reviewer for the WOCN Society and the Journal for WOCN. Her main career focus is on the advancement of wound care through evidence-based research.
The views and opinions expressed in this blog are solely those of the author, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.




