
A Tale of Patience and Persistence: A Positive Outcome Despite Socioeconomic Pitfalls
October 7, 2024
Keywords
Categories
© 2024 HMP Global. All Rights Reserved.
Wound care is a challenging discipline where a myriad of systemic factors needs to be balanced to achieve the ultimate goal of healing. The added peril of working in a safety-net hospital clinic can at times be an additional burden for even the most enthusiastic clinicians. A safety-net hospital, per definition, is an institution with a legal obligation or mission to provide healthcare regardless of the ability to pay.1 These facilities care for many Medicaid beneficiaries and uninsured patients in a particular geographic area.2 In short, resources are limited, and the ability to refer to various specialties is greatly restricted. The mentality I've observed amongst clinicians working in these facilities is to make the best of what is accessible. This brings to mind the quote by Marcus Aurelius, "Our life is what our thoughts make it," or in medical terminology, using our knowledge to create the utmost therapeutic experience possible.
So, with that bit of inspiration at play, a referral came from the infectious disease service regarding an elderly patient with a leg wound that would not heal. This individual had been seen by various clinicians and even by the wound center in the downtown area. All of these events resulted in frustration and a referral back to the safety-net hospital clinic, which the patient not-so-affectionately referred to as "death's doorstep." The patient was very upfront with his disdain for healthcare providers in general and his complete lack of trust in the modern medical establishment. His first words at the start of the hospital wound clinic visit were, "I am only here because my infection doctor nagged me to come one more time, but I do not think you can help me." In response to those very enthusiastic words, the proposal was made to review previous treatment rendered and come up with a plan that we (both patient and physician) can agree upon that serves his best interest.
Details on the Clinical Scenario
The patient is an 87-year-old Caucasian male with a significant past medical history of lymphedema, venous insufficiency, urinary incontinence (Foley catheter in place), chronic anemia, and glaucoma. His right lower leg ulceration had been present for over 3 years with the most current treatment being a "homemade salve of peroxide and baking soda" with an incontinence pad and loose gauze wrap applied. He continues to refuse any wound biopsy or vein mapping and will not tolerate an Unna boot. On clinical examination, his wound is large and irregularly shaped, measuring 11.0cm x 16.0cm x 0.3cm with 40% granulation and 60% fibrotic tissue present. He also had copious amounts of serous-sanguineous exudate without malodor, observed as a CEAP 6 classification with Stage II lymphedema (+ Stemmer's sign, pitting edema, papillomatosis). Recent x-rays showed no underlying osseous involvement, and he did have a slightly elevated white blood cell (WBC) count due to a urinary tract infection being treated with doxycycline. His albumin was low around 3.4g/dL with normal renal function noted.
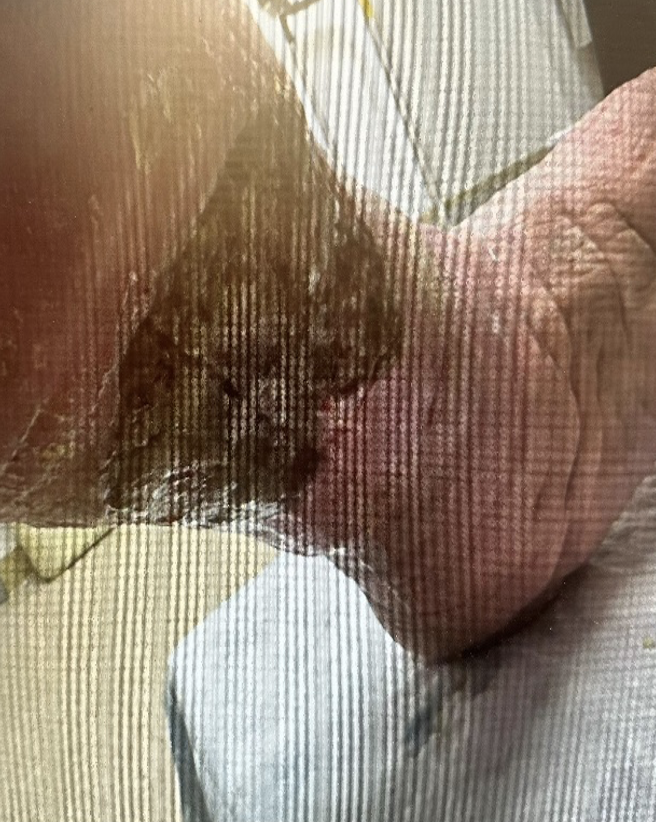
Right leg ulcer-1st visit (May 2024)
Chronic venous insufficiency (CVI) is one of the 4 most common causes of lower limb lymphedema along with cancer treatment in Western countries.3 CVI is a common condition characterized by lower extremity edema with skin changes, along with the risk of ulceration.4 The pathophysiology reflects venous hypertension as a consequence of valve incompetence, destruction or obstruction within the venous system.4 There is as often an overlooked lymphatic component with advanced CVI resulting in lymphatic impairment during the clinical stages of chronic venous disease.3 Prolonged venous hypertension can permanently damage lymphatic architecture, leading to worsening edema, giving rise to dermal abnormalities.3 This compounded insufficiency of both the lymphatic and venous systems makes managing chronic leg ulcerations even more challenging.
Confronting Compression
Compression therapy remains a vital component to the treatment course for both lymphatic and venous disease, with contraindications mainly being arterial insufficiency and severe congestive heart failure (CHF).5 This particular patient was vehemently opposed to compression, having despised his past experiences with Unna boot therapy. The bandaging options at that particular clinic are quite limited with no commercial compression systems available. That being said, creativity is a necessity for success! Thus began the compression bargaining game, and after much back-and-forth banter, we finally reached an agreement. He begrudgingly accepted the use of an elastic wrap from toe level to just below the tibial tuberosity. It was helpful that his wife was an advocate for compression and she regularly participated in his care. The patient refused sharp debridement, so we employed a mechanical method, which he tolerated well. A primary dressing of an antimicrobial foam was applied to assist with the moisture balance with a secondary application of abdominal pads and pre-fluffed gauze. His wife took notes regarding the dressing change protocol, and basic supplies were provided for home dressing changes every 2 days. Weekly visits were not feasible due to the patient's transportation issues, so we implemented a biweekly schedule. Samples of a nutritional supplement were provided along with coupons for purchasing this over-the-counter powder preparation to address his low albumin and to enhance the healing cascade from a nutritional standpoint.
On his second visit to the hospital wound clinic, the patient's demeanor was strikingly different, and he expressed gratitude along with amazement regarding his progress. After 2 weeks of treatment with the antimicrobial foam, secondary dressing with an ace wrap for compression, and nutritional supplementation, his wound had significant signs of healing. The wound on this particular visit measured (1.0cm x 6.0cm x 0.1cm) with 80% granulation and 20% fibrotic tissue, and less serous-sanguineous exudate present.
We continued this same therapeutic protocol, and the patient fully healed after 4 visits (8 weeks in total) to the hospital-based wound clinic. After the ulceration healed, the patient was amenable to wearing compression stockings regularly to prevent ulcer recurrence.

Right leg-fully epithelialized (July 2024)
Overcoming Obstacles
The patient and his wife contacted the Patient Relations division of the hospital, which typically receives complaints, and shared their positive experience in the wound clinic. Their statement reflected that, despite being underinsured, they felt their voices were heard and that they were truly being cared for without contempt or condescension. Having a say in their care plan was very empowering and enabled a bond of trust to be solidified. While our situations may not be ideal, it is within our power to improvise and persevere. There is much to be said about meeting people on their level and going forward together from that point. In the words of Theodore Roosevelt, "Do what you can, with what you have, where you are." This sums up the adventure of providing wound care in a safety-net hospital system.
References
Chatterjee P, Sommers BD, Joynt Maddox KE. Essential but undefined — reimagining how policymakers identify safety-net hospitals. 1. 1>1. Chatterjee P, Sommers BD, Joynt Maddox KE. Essential but undefined — reimagining how policymakers identify safety-net hospitals. New Eng J Med. 2020;383(27):2593–2595. https://doi.org/10.1056/nejmp2030228
2. McNeill E, Cronin C, Puro N, Franz B, Silver D, Chang J. Variance of US hospital characteristics by safety-net definition. JAMA Netw Open. 2023;6(9). https://doi.org/10.1001/jamanetworkopen.2023.32392
3. Dean SM, Valenti E, Hock K, Leffler J, Compston A, Abraham WT. The clinical characteristics of lower extremity lymphedema in 440 patients. J Vasc Surg. 2020;8(5), 851–859. https://doi.org/10.1016/j.jvsv.2019.11.014
4. Senanayake J, Chaudhari S, Haji Rahman R, Madanat S, Tiesenga F. Chronic venous insufficiency and lymphedema with papillomatosis cutis lymphostatica, hyperkeratosis, and skin ulcers: A case report. Cureus. 2023;1–7. https://doi.org/10.7759/cureus.35326
The views and opinions expressed in this blog are solely those of the author, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.

